
As I’ve mentioned before, I am currently working as a medical assistant in pain management. It’s now been almost a month that I started my new job and I love it! I get to work alongside the best pain management doctors in my area and have learned so much in a short amount of time. Last week, I had the privilege of shadowing several Epidural Steroid procedures as well as a Kyphoplasty procedure. It was the coolest thing I’ve seen since tori removal back in my oral surgery days. If you don’t know what a Kyphoplasty is, keep reading because this post is all about it!
What’s a Kyphoplasty?
A Kyphoplasty is a procedure performed to correct vertebral compression fractures (VCF) through the use of polymethylmethacrylate (PMMA) aka bone cement. The leading cause of VCFs is osteoporosis (Cooper et al, 1992), but falling or high risk activities like lifting heavy weights could also lead to a fracture. Due to the nature of the fracture, VCFs can be very painful; the vertebral body collapses causing the patient to lose height in their spine. During the procedure, a hollow needle is inserted into the body of the vertebra through the pedicle. An inflatable balloon is then placed inside, inflated to restore the vertebral height and to create a working channel for the cement to flow into. The entire procedure is guided through a fluoroscope and contrast medium.

Why a Kyphoplasty?
Other treatment options for patients with painful VCFs include non-surgical management (NSM) and a Vertebroplasty procedure. A Vertebroplasty is very similar to a Kyphoplasty. The primary difference is that a balloon is not used to create a working space for the cement to flow into and the cement used tends to have a lower viscosity. Both of these factors increase the most pertinent risk associated with the procedure: bone cement extravasating into the epidural space. Without a working space, the physician doesn’t have as much control of where the cement is flowing into. Also, bone cement viscosity is identified as a decisive guideline influencing leakage in a Vertebroplasty, so using a cement with a higher viscosity reduces the risk of extravasation (Giannitsios et al, 2005). In fact, the incidence of leakage during a Vertebroplasty ranges between 2-67% compared to 0-13.5% for a Kyphoplasty (Denaro et al, 2009). Other risks to consider include heart attack, cardiac arrest and stroke. In addition to surgical procedures, there are also NSM options for patients with VCFs. These include bed rest, pain relief medication and back bracing. Compared to patients who undergo a Kyphoplasty procedure, patients following a NSM treatment plan for VCFs experience less pain relief and improvement (Meirhaeghe, 2013). For these reasons, if a non-surgical treatment is insufficient, a Kyphoplasty is often the preferred treatment option for VCFs.
What are the main indications for the procedure?
- Patients with Osteoporosis
- Patients experiencing intense pain adjacent to the level of the fracture
- Patients diagnosed with a fracture by an MRI, CT or X-Ray
- Patients who failed non-surgical management for at least 4 weeks
- Patients with lesion causing benign and metastatic tumors
Which patients are not candidates for the procedure?
- Patients who did not fail non-surgical management for at least 4 weeks
- Patients with asymptomatic vertebral compression fractures
- Patients with allergies to materials used in the procedure such as PMMA or barium contrast
- Patients with bleeding disorders that are unmanageable
How is the procedure performed?
- The patient is placed on the table, face down with a gown open to the back. The patient’s skin where the needle will be inserted is prepped with an antiseptic solution. Most patients are sedated for comfort and since the procedure is minimally invasive, local anesthetic is primarily used.
- The provider starts by inserting a bone access needle into the area affected to determine the trajectory of the working cannula. Once it’s confirmed through the fluoroscope that the access needle is at the correct location (on pedicle of vertebra), a bone drill is used to create a pathway through the pedicle into the vertebral body.
- Once the pathway is created, a curved-tip osteotome is inserted into the vertebral body and manually curved/directed towards the fracture.
- The balloon is inserted through the hollow needle and inflated to compact the soft porous bone inside of the vertebral body. Doing this not only restores the natural height of the vertebra but also creates a working channel for the cement to flow into. This decreases the chances of the cement flowing to places it shouldn’t flow into and gives the doctor more control of the cement’s trajectory. A contrast is used to visualize the inflation of the balloon and its location through the fluoroscope.
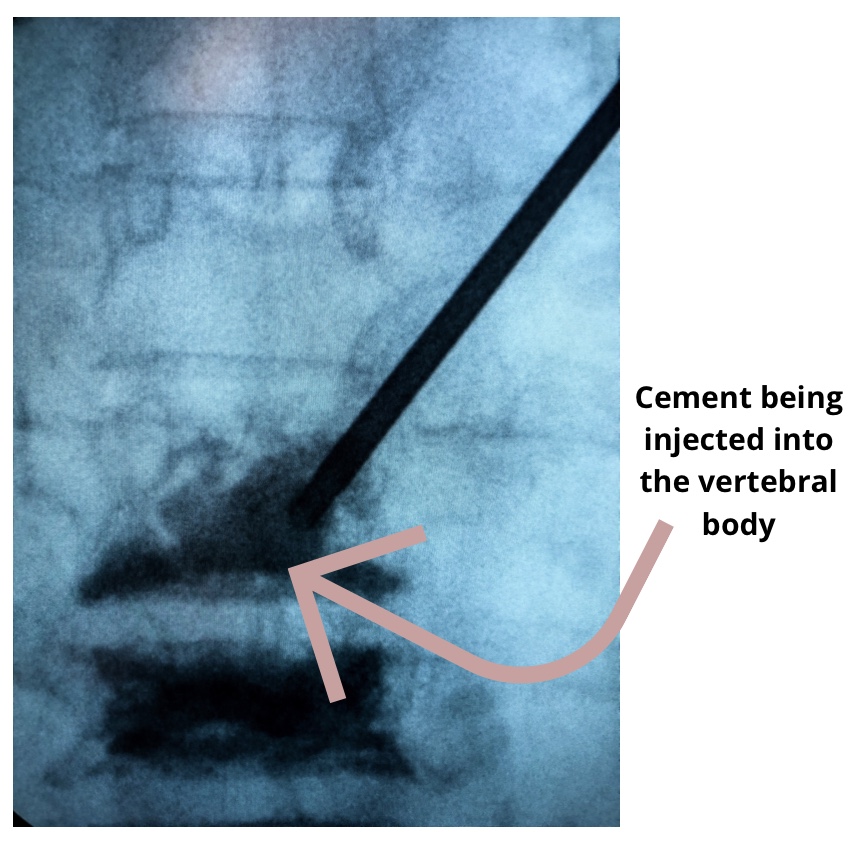
- Finally, the balloon can be removed and cement is injected into the working channel under pressure using a special cement filler cannula. The pressure and quantity of cement being injected is strictly controlled to prevent leakage. The needle is removed slowly and carefully, ensuring the cement is not following the needle forming a “tail.” This is done by waiting for the cement to slightly harden and monitoring its progress through the fluoroscope.
- The needle is removed and the incision is closed with either steri-strips or skin glue. Once the remaining cement on the table hardens, the patient is ready to be moved to the recovery room.
Pictures from the procedure I shadowed:



Works Cited
Giannitsios, D., Ferguson, S., Heini, P., Baroud, G. & Steffen, T. (2005). “High cement viscosity reduces leakage risk in vertebroplasty”. European Cells & Mat 10, Poster No. 314. http://www.ors.org/Transactions/5thCombinedMeeting/0314.pdf
McCall, T., Cole, C., Dailey, A. (2008). “Vertebroplasty and kyphoplasty: A comparative review of efficacy and adverse events.” Current Reviews in Musculoskeletal Medicine, Vol. 1: 17-23, doi: 10.1007/s12178-007-9013-0. https://link.springer.com/article/10.1007/s12178-007-9013-0
Meirhaeghe, J., Leonard, B., Steven, B., Jonas, R. & John, T. (2013). A randomized trial of balloon kyphoplasty and nonsurgical management for treating acute vertebral compression fractures. Spine, Vol. 38(12): 971-983, doi: 10.1097/BRS.0b013e31828e8e22. https://pubmed.ncbi.nlm.nih.gov/23446769/
Denaro, V., Longo, U., Nicola, M. & Denaro, L. (2009). Vertebroplasty and kyphoplasty. Clinical Cases in Mineral And Bone Metabolism: The Official Journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases, Vol. 6(2): 125-130. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2781232/

Leave a comment